myHIN Blog
Category: Health Issues Articles

July 14, 2013
Representations of Black Womanhood: Implications in Health
Miami University
Doctoral Candidate
The prevalence of chronic disease for African Americans is substantially higher than their white counterparts. According the National Health Statistics African Americans had higher rates of hypertension, diabetes, and obesity (U.S. Department of Health and Human Services [HHS], 2010). In addition to having a greater risk for chronic disease African Americans experience more complications and endure greater rates of mortality. Although current data indicates that there have been improvements in mortality rates, life expectancy, and disease prevalence, disparities between the races are still substantial.
In the United States data on health disparities is rarely presented in an intersectional manner, edifying race, class, and gender (Kawachi, Daniels, and Robinson, 2005). It is through the use of controlling black female images that the interpellation occurs and health disparities are perpetuated. When individuals connect with images and do not engage them critically we allow dominant hegemonic representations to colonize our minds, shaping our assumptions about ourselves and others (Gauntlett, 2002). The connection between how black women were viewed and the implications it might have on health policy, health education, and individual interaction with the healthcare system has never been directly addressed in health disparity literature. Researchers tend to focus on issues of access emphasizing availability of adequate health insurance, culturally competent healthcare providers, and medical centers (Smedley, 2003). While, addressing issues of access is an important component in reducing health disparities controlling for these factors health disparities still remain.
Controlling for variables such as income, health insurance, and access provides minimal impact on the health of African Americans when matched to white counterparts, so the question must be asked, “why do black women have so many health problems relating to obesity, diabetes, and heart disease?” What part does racist and classist ideological beliefs have on health outcomes? Focusing on the short-comings of health education in regards to enacting positive change in minority communities brings one to the study of black female images. It is through these images that black female identity is viewed and formed, shaping intra-personal and interpersonal development and interaction. The intrapersonal deals with the psychology of the individual delving into how identity and self concept is conceived, and this is important for understanding of how the individual may view self, which provides insight into potential motivations for self-care.
The construction and perpetual use of misrepresentations of black womanhood has left an indelible mark on the American healthcare system. As an African American female the relegation to subservient and deviant roles is assured; for the female staring as the jezebel or the mammy is the best that can be expected. Reiterations of these representations play out on the news, television shows, magazine covers, and movies. Visual, auditory, and social text displaying these controlling images almost seem inescapable. Text provides a specific discourse about race, class, gender, and sexuality, and while the viewer is able to pick and choose the text that he are she interacts with the process of mediating the messages that are received is not entirely possible. Living in a perpetuate world of performance due to the white gaze African Americans loss ‘self’ taking on the embodiment of the oppressor’s image of other. This internalization of mammy or jezebel requires the African American woman to perform her ascribed role. The role of the mammy as it relates to self-care does not allow space for the black woman to acknowledge her mental or physical health. The role of the mammy is to care for the needs of others and sacrifice herself for the good of others. The jezebel on the other hand has no real regard for her health or that of anyone else. Her function is to seek pleasure and satisfy her temporal desires. Both images construct identities disconnected from self in the sense that one is unable to be attuned with what is needed to become and remain well. Likewise, many of the other representations of black womanhood suffer from this lack of attunement due to being conflations of old representations of slavery, reclaimed oppressive images, or images constructed in binary opposition to hegemonic representations of white superiority.
Resolving health disparities becomes far more than simply providing education and access, it hinges on identifying racism and acknowledging the cultural and political power that racist images and narratives have in our social ecological spheres (Shavers, 2006; Sanders-Phillips et. al.). Understanding the intentions and motivations behind health behaviors of the marginalized comes with deep exploration of those oppressing acts and representations that serve to colonize and recolonize (Speight, 2007). A stripping away of oppressor hegemonic cultural narratives must be undertaken and empowered counternarratives constructed from more authentic afrocentric spaces must occur.
Follow us on Tumblr tumblr.myhealthimpactnetwork.org
Follow us on Twitter @myhealthimpact
Share

May 06, 2013
The Evolution of a Sneakerhead
As the days dwindle away and graduation finds its way closer, a lot of thoughts have been running through my head. Thoughts primarily centered on my college experiences and how those moments have shaped me into the person I am today. Being a part of the myHealthImpact project has meant a lot to me, from gaining tangible skillsets to traveling across the country to promote our efforts. Although my obsession for simplicity and design drove my involvement with myHealthImpact, it was this representation of realizing a problem and attacking it head on with a unique solution that initiated my thoughts with respect to footwear.
As a child I was always fascinated with various types of sneakers. I wasn’t interested in wearing ‘regular’ or ‘basic’ shoes. I was more content with the latest and greatest Nikes, Jordan’s, and yes even Fila’s! I would beg my mom until she gave in and purchased my favorite pair of sneaks; but for some reason I was never completely satisfied. As the most expensive shoes felt uncomfortable and irritated me when I walked. This was evident because I had already been diagnosed with femoral antersion, or walking pigeon-toed, a common childhood orthopedic condition.
For a short time, I also wore shoes with braces, which I despised. While in middle school, I faced additional foot problems that made it difficult for my feet to stay on the foot bed of most sneakers. As a freshman at NCSU the foot problems ensued and further measures were taken such as creating a mold that I would wear in my shoes to provide comfort as I walked around campus. Currently, I have to engage in daily rituals by performing various foot exercises to ease the pains I may encounter during the day. Needless to say I have endured enough.
Despite my constant foot problems, for those who know me, I have been a lover of sneakers from the beginning of time. My devout following to rocking the latest kicks really took off when I entered college and met a small group of individuals who also shared this same passion. After accumulating dozens of shoes and even hosting the first ever sneaker showcase titled "Sneaks and Beat's' back in 2010, I still felt the need to do more. Now that I have officially hanged up my sneaks and done a lot of reflection, I have been toying with the idea of ending my retirement and refocusing my career on designing athletic footwear in conjunction with the medical field for optimal foot health.
Post graduation, I hope to take my experiences and turn it into a career filled with passion while helping others along the way. Thus, my involvement as an Undergraduate Researcher for this project has tremendously influenced me to pursue @myHealthImpact.
Follow us at tumblr.myhealthimpactnetwork.org (Tumblr)
Follow us on Twitter @myhealthimpact
Share
April 20, 2013
Mass Media, Sex, and the HIV Chat
By the time I was 16, I was already aware of what condoms were, how they were used and who used them. As a 20 -year-old graduating college senior, I look back on all I know about HIV. In order to address the discussion of HIV among teens, we must also talk about the sex discussion first because they are related. For one thing, I know that my parents had little to do with the discussion about sexually transmitted diseases. A curious kid at 16, I was also an avid ‘TV-watcher”. Like most of my African-American peers, we always discussed how tv shows like Flavor-of-Love, the Real World and Desperate Housewives influenced us on our view of sex. Because HIV is a sexually transmitted disease, there is much to be said about the virus. My peers and I also know that TV, as a form of mass media sends messages to teens all across the world. Positive messages. Negative messages, perpetuating stereotypes and false information are what is shown to people everyday. Mass media, as defined by sociology dictionary is forms of communication designed to reach a vast audience without any personal contact between the senders and receivers. Examples would include newspapers, magazines, video recordings, radio and television.
As a broadcast journalism major, I was taught that journalism, in lieu of mass media is the fourth estate. The first three estates being the Legislative, Executive and Judicial branch of the government. We are the gatekeepers of information. When I think of a gatekeeper of information, I think of a safeguard. A safeguard is someone who guards, protects and sensors something in a positive or negative way. During my teenage years, the only time I saw HIV awareness or discussion about HIV on TV was during World Aids Day and on December 1st, which is national HIV testing day. The media has more messages of free sex, sex with multiple sex partners and having sex with the absence of love, commitment or respect. There are more reality shows and sitcoms about those topics than shows that address safe sex, monogamy or abstinence. This poses as a threat to the teenage discussion of HIV because they are receive mixed messages that can lead to ignorance. For instance, some teens believe AIDS is the same as HIV, which is false. I’ve also witnessed a discussion at the university level where a student said, “ I need to take an AIDS test”, which is highly inaccurate. Where does the inaccuracy come from, one might add? I am reminded of the huge responsibility TV plays in the discussion of HIV among teenagers. To me, there is no discussion of HIV. I do not feel that the TV industry does a good job of informing the public of the causes and symptoms of HIV/AIDS. For one, I believe that many teens do not know the difference between HIV and AIDS, and that discussion is where the media, as a fourth estate should start.
Follow us at tumblr.myhealthimpactnetwork.org (Tumblr)
Follow us on Twitter @myhealthimpact
Share

April 15, 2013
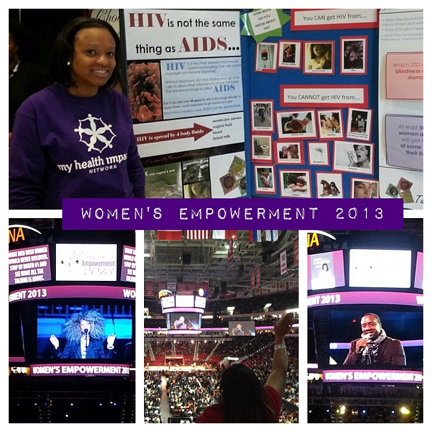
Women’s Empowerment 2013
Last month, the PNC Arena experienced something that only happens once a year. By 11am, over 8,000 women, of all ages and races, filled the arena and were eager to be empowered! The spirit was overwhelming.
The first person to empower me was Bishop T.D. Jakes. The title of his sermon was “Lord, don’t give me anything I can’t handle”. Here are a few notes that I took:
- God is not fair
- If I couldn't handle it, He wouldn't have given it to me!
- Fear will shut down your instincts and steal your time
- Success is intentional!
The last point stuck out to me the most. Success becomes intentional the minute you set a goal to do something. If all goes well, you will make it to a place called success and look back at your goals ready to check one off of the list. Don’t think that you are just “lucky”. Everything happens for a reason!
After this very inspirational word, I decided to get to work for myHIN! Jeremy and I went around to the vendor’s area and began passing out our business cards and telling people about our project. As I walked around, I noticed that there was a booth set up specifically for HIV/AIDS and they had information and stickers from the Greater Than AIDS movement to pass out! I was very pleased to see this booth amongst the people selling clothes, jewelry, and artwork. It was a perfect location to spread the message.
It was great to be amongst so many women who came together for one goal: to be empowered! I can really say that after the Black Men Revealed Panel, Wendy Williams, and Erykah Badu’s performance, I left PNC Arena better than I came! I was very excited that once again, I was able to combine my love for music with my interest of helping put an end to HIV/AIDS.
Below is a picture that sums up my day at the event!
Follow us at tumblr.myhealthimpactnetwork.org (Tumblr)
Follow us on Twitter @myhealthimpact
Share

April 10, 2013
The Problem with Black Women’s Health
Dominant. Independent. Bitter. Empowered. Manipulative. “I can do bad all by myself”. Superwomen. Stubborn. In denial. Ladies, what do these characteristics describe? These words or phrases are often used to label African American women. Whether we categorize these features under positive or negative connotations, there is unfortunately some truth behind every single one of them. African American women are hard- working, dedicated, educated professionals but we tend to put everyone and everything before ourselves. We want the best for our families and friends, which tends to become our overall mission of life, and forget about our own personal image and health. In many cases, African American women are single parents or just self- reliant individuals who metaphorically develop stern, powerful mindsets as their defense from real and perceived attacks. We go hard on ourselves since we automatically fall within the lower rank in American society; being classified as “double wammies” since we are female AND of the racial minority.
The number one health-related issue that black women deal with is cardiovascular disease. According to the National Stroke Association, one half of all African American women will die from stroke or heart disease. The death rates from heart disease and strokes for African American females are double those of White and Hispanic females. Our culture also tends to continuously struggle with health problems associated with obesity and high blood pressure. From overworking ourselves and fighting sleep, to insisting that we are in good health (bitterness), all of these cultural aspects play a role in our refusal of medical assistance when we need it most.
“Too many of us are just as crazy, walking (or running) around in denial, ignoring signs (headaches, exhaustion, dizziness, vision changes, weakness, numbness) that should send us to the doctor, not to the office or the car pool or off on that next ‘all important’ business trip. We are in denial about the real impact of our obesity, our smoking, drinking, and lack of exercise…all women should remember that whatever power we each possess is rooted first and foremost in our health. We work so hard to control so much and we’re always up for a challenge. Fine! Here’s a challenge! Commit to spending more time and attention controlling—and caring for—yourself.” (Caroline Clarke, Black Enterprise: Wealth for Life)
Share

April 06, 2013
Ice Cold Brothers, Bowl for Babies
On Thursday March 14th 2013, the Infamous Eta Omicron Chapter of Alpha Phi Alpha Fraternity, Inc. hosted their 6th annual “Bowling for Babies Tournament”. This tournament began in 2007 as an innovative way to raise monetary funds for the March of Dimes Foundation. The March of Dimes Foundation is a non-profit organization founded by President Franklin D. Roosevelt to prevent infant mortality and Polio along with improving the health of babies as well as mothers. The March of Dimes Foundation is a national initiative of Alpha Phi Alpha Fraternity, Inc. and has been a major philanthropic project in which the fraternity has been engaged in for years. The turnout of the event was awesome and it continues to be a success every year.
As the President of the Eta Omicron Chapter at North Carolina State University, we really take this event seriously and we are striving to have a greater impact in educating the student body on infant birth defects. Check out Professor Gore’s article entitled, “So what’s the real deal here?” This article discusses the survival of a baby born to a mother who was HIV positive. The significance of this baby is that it was not born with the virus. Besides it being a miracle, the credit for the baby’s survival can be accredited to early detection. By being properly educated and understanding the resource.
In the future, we plan to use different method’s to increase the awareness of infant mortality, birth defects, and even the latest news of the baby being cured from HIV. The event provides the student body with information that can improve or save a life. We look forward to continuing the legacy of “Bowling for Babies” for decades to come. All proceeds made from this event are donated directly to the March of Dimes Foundation. By bowling a ball, it can save a life!
Share

February 12, 2013
Let’s Talk About Sex Because Sexual Health is Important
A study conducted by researchers at the University of Chicago found that only 60% of OBGYN’s ask questions about their patient’s sexual activities sex during medical visits. They also found that many OBGYN’s knew very little about their patients’ sexual behavior, sexual satisfaction and even sexual orientation.
Why are women not discussing their sexual lives with their physicians? According to the researchers, the reasons may be that 1) physicians do not ask and 2) patients do not bring their sexual activities up as points of concern.
Discussing sexual health with your physician is important, because changes in sexual functioning or behaviors can help the doctor identify other health problems that could escalate if left diagnosed and untreated. For example. HIV/ AIDS tests are also not always routinely given to all women and when a doctor knows about your sexual health, they may know when to recommend you take one. This is particularly important as rates of HIV infection among African American and Hispanics women are much higher than those found in white women. Sixty-four percent of women with HIV are Black. And HIV infection is among the top 10 leading causes of death for Black females.
Some tips to help you have discussions about your sex life with your doctor are.
- Find a doctor you can trust. Many women settle for the provider that is given to them by their insurance company, but finding a good doctor is sometimes like dating. You must think of what characteristics and work practices you need in a provider that will compliment your needs. If you cannot trust you doctor, you might not feel comfortable discussing everything with your doctor and you may be putting your health at risk. If one relationship is not working, find a new one.
- Do not limit your discussions of sexual behavior to your OBGYN, you might find that you are more comfortable talking about your sex life with your primary care doctor. You might also feel more comfortable discussing some concerns with a therapist or psychological professional. For example, concerns such as coping with sexual abuse, suspecting that your long-term partner is unfaithful, becoming dissatisfied with sex or having multiple simultaneous sexual partners can all affect your health. For each of the above concerns, your health care provider or team can provide support and recommend appropriate treatments.
- Keep track of your sexual behavior, functioning and questions. Bringing a record of concerns related to your sexual health to your physician can help start the conversation and may help your diagnosis better treat you. Remember, it is OK to ask that certain types of information remain conversational and not become parts of the medical record.
- Seek care and stay up to date with routine care activities. If you have a long-term relationship with the same care provider, it will be easier to discuss your sex life and it will be easier for that provider to identify changes in your sexual behavior and find solutions to help you.
Resources:
Sobecki JN, Curlin FA, Rasinski KA, Lindau ST. What We Don't Talk about When We Don't Talk about Sex1: Results of a National Survey of U.S. Obstetrician/Gynecologists. The Journal of Sexual Medicine. 2012;9(5):1285-94.
Dr. Heather Watts, a liaison member to ACOG's Committee on Health Care for Underserved Women
Most women are infected with HIV through heterosexual sex. Some women become infected because they may be unaware of a male partner’s risk factors for HIV infection or have a lack of HIV knowledge and lower perception of risk. Relationship dynamics also play a role. For example, some women may not insist on condom use because they fear that their partner will physically abuse or leave them. (source: http://www.cdc.gov)
http://www.wordle.net/show/wrdl/6304616/Sexual_functioning_surveys
Share
February 11, 2013
Philadelphia High Schools Promote Safer Sex
“What has the world come to?” is often a question that floats through my mind as I read the news. Being an African American woman in a predominately Caucasian class is unsettling when the teacher reveals a chart of health statistics and African Americans are highest at risk for practically every sexually transmitted disease. Black women were second in comparison to black men in terms of early death rate; however, African American women are the highest ethnic/ gender group overall to contract sexually transmitted diseases (STDs). Why is this so? One reason that comes to my mind is that females are more likely to go get tested than males. Furthermore, why is the percentage rate of these diseases high in the black community particularly?
Unfortunately, most STDs are contracted and spread by our young people (teenagers & young adults). In my hometown, Philadelphia, STDs are spreading rapidly, especially in the public school system. The mayor, Michael Nutter, noticed the dangerous trend amongst these students and came to a controversial conclusion to disseminate condoms at public schools without parental consent. The majority of public high schools have condom dispensers located in a nurse facility to supply all students with free condom protection. When I was in high school, condoms then were available to students, but we had to have parental consent. This new policy may help solve the problem of the spread of STDs, but created another. Parents are now questioning why their children’s school is “giving them the right to engage in sexual activities”. For more information on this new policy, see http://sexetc.org/
I perfectly understand both sides of the argument. However, I believe that students will choose to have sex regardless of whether or not condoms are free or not (personal decisions). The school system is just educating kids to have safer sex if they are going to have sex at all. The choice to abstain from sexual activity is still available. However, sexually active teens and young adults in the Philadelphia area can http://takecontrolphilly.org/ to find where to go to get free condoms.
Share your thoughts with us. Let us hear from you via a blog comment or on Twitter @myhealthimpact.
Share
February 04, 2013
The “Other Red”
Friday marked the first day of Black History and Heart Disease Month! It is not completely ironic that these two months take place simultaneously, considering the impact heart disease has had on the Black community. Heart Disease is the number one killer of women, causing 1 in 3 deaths each year [1]. Of African-American women ages 20 and older, 49 percent have heart disease. This is very alarming to me considering both sides of my family have a history of women with high blood pressure.
On Friday, the Kappa Omicron chapter of Alpha Kappa Alpha Sorority, Incorporated hosted ‘Pink Goes Red’, a Zumba event used to raise awareness of heart disease and give attendees an opportunity to take action towards combating this condition. Other than the fact that I love Zumba, I really wanted to attend because I am a strong advocate for the ‘Go Red For Women’ campaign. As a member of the Mu Omicron chapter of Delta Sigma Theta Sorority, Incorporated, I initiated the chapter’s philanthropic efforts to go towards the ‘Go Red For Women’ campaign since our sorority was the first to join the American Heart Association through this effort. Since 2011, we have donated over $300 to the campaign through hosting various events such as ‘Breakfast In Red’, a pancake breakfast which raised money and awareness for Heart Disease. This year, we will have a table set up on the brick yard at NC State during our annual Crimson and Cream Week where we will spread information about heart disease and raise money to donate to the campaign.
A lot of people know how much the color red means to me, especially since my first car, CD player and cell phone was red. My high school and university’s primary color is red, and my sorority’s color is also red. However, they don’t know that red is also important to me because of heart disease. My great-grandmother passed away because she had not taken her blood pressure medicine for several days leading up to her death. Knowing this and learning about the other diseases that are prevalent in my family has really inspired me to lead a healthier lifestyle by watching what I eat and exercise.
Although My Health Impact Network has an initial focus on HIV/AIDS prevention and awareness, we cannot forget about ‘the other red’ - heart disease. People with HIV have more than four time the risk of sudden heart attack as their uninfected peers, according to Dr. Priscilla Y. Hsue [2].
Sources:
[1] Go Red For Women
[2] Health Attacks in HIV Patients -- NY Times
Share
September 10, 2012
“You Ain’t Crazy: It’s Your Mental Health!”
On Thursday, August 30th, Dr. Payton gave a presentation on campus titled ‘You Ain’t Crazy: It’s Your Mental Health’ where she discussed mental health issues in the African-American community. What stuck out to me the most was the video she showed featuring Terrie Williams where she talks about her book “Black Pain: It Just Looks Like We’re Not Hurting”. Williams talks about how people think they are the only one who is going through something so they keep things bottled in and suffer from depression, hyper tension, and heart disease; or it will come out through self-medicating, gambling, sex, risk behaviors, etc. Risk behaviors can only increase the chance of being exposed to HIV.
For some strange reason, in our community, when we are suffering from something such as depression, we don’t go and get help. Instead, we turn to a friend who ends up giving us bad advice or just decide to seek a spiritual source to resolve our problems. While I am not knocking the latter, sometimes it is good to keep mental and spiritual health issues separate. Unfortunately, I am speaking from experience.
Last semester I had things going on with my family that I had never experienced before and I didn’t have time to react properly. I used my school and extra-curricular activities as a way to block everything out until one day it caught up with me. I literally woke up crying. I didn’t go to class that morning (which added to my stress) and I reached out to one of my sorority sisters who I am close with. Having experienced depression before, she forced me to go to the University Health Center to seek counseling. I was skeptical at first, but I figured it wouldn’t hurt to talk to someone who was a professional. I went to the Health Center and was told that I needed to set up an appointment. I was upset because I didn’t want to wait to talk to someone in seven days; I needed someone at that moment. I was afraid that my natural habit of pushing things away would hinder me from receiving proper help. In any case, I set the appointment and returned a week later. Unfortunately, the counselor was not helpful, but I was proud of myself for taking the initial step.
When I told certain people in my family that I went to see a counselor their response was ‘what do you need to do that for?’. I responded ‘to make sure I don’t go crazy!’. I also told them that I wanted to find another counselor and begin seeing them regularly, again they asked ‘what do you need to do that for?’. I believe that counseling can help you receive an unbiased opinion on how you should move forward. A counselor does not give you advice based on experience. They give you advice based on clinical research that can help you control your reaction to events that you can’t control. Can you control risk behaviors?
If you’re reading this and you have something that you are dealing with, seek help. More than likely you are not alone in the matter. If you need motivation, watch the video below featuring Terry Williams who also gives her personal testimony about battling with depression.
For up-to-date information, follow @myhealthimpact on Twitter!
Share
In Partnership with: Poole College of Management, College of Humanities and Social Sciences, National Science Foundation, Penn State
Take Action, Get Tested: Find Your Local Testing Center Why Get Tested?