BlogSpot

July 21, 2013
Why Health? Dad and Me
On May 9, 2012, a 44-year old, African-American male that exercises regularly and eats pretty well suffers from a heart attack. This man is my Father, my Dad, and my best friend. To see him, the man that has given up so much for me, laid in a hospital bed helpless shocked me. I never stopped to think, not even in my wildest dreams, that anything like that could happen. Tip 1: no one is invincible. This situation helped kick start my healthy lifestyle walk as well as wanting to encourage others to do the same. Hopefully this isn’t speaking badly of me, but before and now just a little over a year later, my Dad is more in shape than me. Seeing someone that does more than you in the gym suffer from a heart attack is scary.
My Dad constantly reminds me that we have the same blood running through our veins; we are one in the same and I must be completely aware of the health issues that could arise if I don’t take care of myself. I may pout as he reminds me of this as I lift a burger into my mouth or don’t want to get out of bed to workout, but he’s right and I know he is. I’ll call him my built in accountability partner. Tip 2: An accountability partner is extremely helpful. Get one of those!
To see someone I love in a situation like that, motivated every inch of me to help others as well as myself from having to experience the same thing. My goal is to lift as I climb in my journey which involves teaching, getting the information out there, and getting people involved not just with the project but actively whether it’s walking, running, eating healthy or (hopefully) a combination of it all. So I’ll leave you with Tip 3: GET INVOLVED. Being involved with MyHealthImpactNetwork has helped me stay on course. I can’t possibly motivate others to get healthy if I’m not doing so myself. To speak contradictions is something I choose not to do.
As I look around my community (college and hometown), the information is there but is it being put out there in a way that it is understood or in an outlet used by those it needs to be reached? MyHealthImpactNetwork does that and I’m making myself a part of that. I feel like it’s my duty.

Share

July 14, 2013
Representations of Black Womanhood: Implications in Health
Miami University
Doctoral Candidate
The prevalence of chronic disease for African Americans is substantially higher than their white counterparts. According the National Health Statistics African Americans had higher rates of hypertension, diabetes, and obesity (U.S. Department of Health and Human Services [HHS], 2010). In addition to having a greater risk for chronic disease African Americans experience more complications and endure greater rates of mortality. Although current data indicates that there have been improvements in mortality rates, life expectancy, and disease prevalence, disparities between the races are still substantial.
In the United States data on health disparities is rarely presented in an intersectional manner, edifying race, class, and gender (Kawachi, Daniels, and Robinson, 2005). It is through the use of controlling black female images that the interpellation occurs and health disparities are perpetuated. When individuals connect with images and do not engage them critically we allow dominant hegemonic representations to colonize our minds, shaping our assumptions about ourselves and others (Gauntlett, 2002). The connection between how black women were viewed and the implications it might have on health policy, health education, and individual interaction with the healthcare system has never been directly addressed in health disparity literature. Researchers tend to focus on issues of access emphasizing availability of adequate health insurance, culturally competent healthcare providers, and medical centers (Smedley, 2003). While, addressing issues of access is an important component in reducing health disparities controlling for these factors health disparities still remain.
Controlling for variables such as income, health insurance, and access provides minimal impact on the health of African Americans when matched to white counterparts, so the question must be asked, “why do black women have so many health problems relating to obesity, diabetes, and heart disease?” What part does racist and classist ideological beliefs have on health outcomes? Focusing on the short-comings of health education in regards to enacting positive change in minority communities brings one to the study of black female images. It is through these images that black female identity is viewed and formed, shaping intra-personal and interpersonal development and interaction. The intrapersonal deals with the psychology of the individual delving into how identity and self concept is conceived, and this is important for understanding of how the individual may view self, which provides insight into potential motivations for self-care.
The construction and perpetual use of misrepresentations of black womanhood has left an indelible mark on the American healthcare system. As an African American female the relegation to subservient and deviant roles is assured; for the female staring as the jezebel or the mammy is the best that can be expected. Reiterations of these representations play out on the news, television shows, magazine covers, and movies. Visual, auditory, and social text displaying these controlling images almost seem inescapable. Text provides a specific discourse about race, class, gender, and sexuality, and while the viewer is able to pick and choose the text that he are she interacts with the process of mediating the messages that are received is not entirely possible. Living in a perpetuate world of performance due to the white gaze African Americans loss ‘self’ taking on the embodiment of the oppressor’s image of other. This internalization of mammy or jezebel requires the African American woman to perform her ascribed role. The role of the mammy as it relates to self-care does not allow space for the black woman to acknowledge her mental or physical health. The role of the mammy is to care for the needs of others and sacrifice herself for the good of others. The jezebel on the other hand has no real regard for her health or that of anyone else. Her function is to seek pleasure and satisfy her temporal desires. Both images construct identities disconnected from self in the sense that one is unable to be attuned with what is needed to become and remain well. Likewise, many of the other representations of black womanhood suffer from this lack of attunement due to being conflations of old representations of slavery, reclaimed oppressive images, or images constructed in binary opposition to hegemonic representations of white superiority.
Resolving health disparities becomes far more than simply providing education and access, it hinges on identifying racism and acknowledging the cultural and political power that racist images and narratives have in our social ecological spheres (Shavers, 2006; Sanders-Phillips et. al.). Understanding the intentions and motivations behind health behaviors of the marginalized comes with deep exploration of those oppressing acts and representations that serve to colonize and recolonize (Speight, 2007). A stripping away of oppressor hegemonic cultural narratives must be undertaken and empowered counternarratives constructed from more authentic afrocentric spaces must occur.
Follow us on Tumblr tumblr.myhealthimpactnetwork.org
Follow us on Twitter @myhealthimpact
Share

July 07, 2013
Book Review – Living & Dying In Brick City
I was listening to NPR some time in early February 2013 and happened to catch Dr. Sampson Davis discussing his then new book, Living & Dying In Brick City. I was struck by Dr. Davis’ candor about his experiences as an emergency medicine physician in his beloved Newark, New Jersey. What I heard was a passion for community with compassion for patients. I remember this same spirit of Dr. Davis and his two life-long friends (who form the Three Doctors Foundation) in their book talk on The Pact at a local bookstore 10 years ago.
I tweeted takeaways and lessons learned from each of the Living and Dying chapters. Dr. Davis discusses his own family including watching his sister suffer from drug addition and complications associated with AIDS. He discusses topics of Black women and image, obesity, stroke, sexually transmitted infections, heart disease, sickle cell anemia and diabetes – all disproportionally impacting the Black community. OMG, I learned A LOT about sickle cell by reading the “Hidden In Plain Sight” chapter, and the disease “runs” in my family.
Health In Your Brick City?
Yes, the book offers the statistics for the data driven, but the power is in the stories offered. The stories offer context and intersectionality.
Without context, the numbers do not offer a complete picture.
By using social media and other technologies, I have communicated to the myHealthImpact (myHIN) Nation about the lessons offered by Dr. Davis. myHIN Nation, what will you do to empower and influence your “Brick City”? Raise your voices and share your thoughts.
Follow us at tumblr.myhealthimpactnetwork.org (Tumblr)
Follow us on Twitter @myhealthimpact
Share
June 25, 2013
Holding a Friend Accountable
Tired. Stressed. Frustrated. In a recent telephone discussion, this is how a dear friend described her life over the last six months. Brenda (name changed to maintain anonymity) and I have been friends since we were two years old! I know. How unusual for two people to maintain strong ties for what truly is a lifetime. With the stressors of career discontentment, professional anxiety and a demanding personal life, Brenda cares for her children, aging parents, job, husband and grandchildren. She postures to do and be all things to all people – as many women, Black women historically, have done and oftentimes continue to do. Despite these many roles, Brenda (like many of us) have been said by some scholars to exist at the margins.
More importantly, Brenda’s health (our health) suffers from the intersectionality of not only race and gender, but personal and professional roles she (we) has. During our telephone chat, Brenda began to share her frustrations with me. Goodness knows that I have unloaded on her before. Our friendship is based on listening rather than judging wherever we are in life. Brenda told me:
“I have not been sleeping, and the weight is not dropping. Crazy stuff at work..crazy stuff at work. Just tired.”
I decided to hold my friend accountable and replied,
“What are you doing for you? Walk and start with 30 minutes today. Tomorrow is not promised. Start today, and text me after you have completed the walk.”
For the last 10 days, I text Brenda to ask: “What time is your walk?” So far, so good. She is walking daily and starting with 30 minutes. She has cut her food portions, added more vegetables to her meals and told me: “It (the walk) was hard. Very out of shape. Lol! But I love your encouragement”.
….Holding a friend accountable as I know she will do the same for me. Together, we are working to stop the “tired of being tired” mentality.
Follow us at tumblr.myhealthimpactnetwork.org (Tumblr)
Follow us on Twitter @myhealthimpact
Share

June 17, 2013
Girl, They Be Tryin’ to Bring Us Down!
I filed for divorce in 2008. Two years later my world was turned upside down when the divorce was finalized. It’s not like I didn’t see this happening – I initiated the break up. However, so much of my identity was caught up in being a wife, a mother, a professor. I forgot how to be me!
While I experienced many dark and depressing days over the past few years as a single black woman, I also turned introspective and thought a lot about what I wanted to do with my life. One of the greatest lessons learned is that I am an intelligent, beautiful, successful Black woman who deserves to be loved.
Music by Black women really helped me to get my head right. I would sing along with Remy Ma’s Conceited: “You gotta have the mind state like ‘I’m so great’. Can’t nobody do it like you do. Miraculous. Phenomenal. Ain't nobody in here stopping you. Show no love cause you what's up. Look at ya self in the mirror like ‘What the f*ck!” (That was my theme song ya’ll.) I also put Missy Elliott’s Work It in heavy rotation: “If you a fly gal, get your nails done, get a pedicure, get your hair did.” And, there was the independent women that Destiny’s Child sang about: “The house I live in – I’ve bought it. The car I’m driving – I bought it. I depend on me.”
Yet, while I gained confidence in my physical appearance and could take care of myself financially, I yearned for a partner who would protect and care for me. I realize that this fundamental desire to be seen as beautiful and loved seemed to go against the dominant ideology of the Black women’s identity. Damn, I thought, why is it so hard for Black heterosexual women to be loved and protected by a man?
I believe that part of the reason is that everyone’s trying to define us, limit our dreams and expectations. Girl, they be tryin’ to bring us down. Patricia Hill Collins (1999, p.167) writes, "Called Matriarch, Emasculator, and Hot Momma. Sometimes Sister, Pretty Babe, Auntie, Mammy, and Girl. Called Unwed Mother, Welfare Recipient, and Inner City Consumer. The Black American Woman has had to admit that while nobody knew the troubles she saw, everybody, his brother and his dog, felt qualified to explain her, even to herself."
These stereotypical images ascribed to Black women are often used to perpetuate the dominant group's ideology of Black women's inferiority. There’s a perception that Black women don’t deserve the pampered life. Society is used to seeing Black women as downtrodden, angry, domineering, ratchet, promiscuous, and fiercely independent. We are constructed as less attractive than women of other races and ethnicities. Rarely are we afforded the luxury of being feminine, protected, intelligent, and genuinely happy. We are dying unnecessarily because we take on everyone else’s problems and give our all to loved ones, while ignoring our own personal needs.
Our survival depends upon on our rejection of stereotypical images. When we refuse to accept others' definitions of our blackness and our femaleness, we break down the negative forces that challenge our successful and peaceful existence. We need our own self affirming definition of our identity as Black women.
How do we begin to redefine ourselves, and become healthier and happier? I offer a piece of advice.
We have to allow ourselves to be pampered and loved by dependable men who have demonstrated that they are worthy of our trust and loyalty. This “I don’t need a man!” attitude is killing us. There is no shame in asking for help and letting others take care of you sometimes. I can’t even explain how wonderful it feels to finally sit back and let someone else take the lead sometimes. It’s okay to depend on someone else to give you what you want (sorry Beyonce, Kelly and Michelle). However, in doing so, we must maintain our standards and expectations without becoming doormats to others in our lives.
Black women cannot carry everyone’s load. We need to set some healthy boundaries and demand reciprocity in our romantic relationships. We need to learn how to stop investing ourselves into men who do not respect us, show us appreciation, or take but never give in return. Black women should not settle for any partner who undermines her intelligence, trust, and personal accomplishments. Our partners should protect, provide and pamper us - not try to bring us down.
Ladies, create your own labels. Find your own beauty and confidence. Put yourself in places and situations where you will meet positive people. Never lose faith that the loving relationship that you deserve is within your grasp.
Follow us at tumblr.myhealthimpactnetwork.org (Tumblr)
Follow us on Twitter @myhealthimpact
Share

June 11, 2013
The Taboo Topic in Student Communities
I found My Health Impact Network through a twitter chat. As an organization focused on targeting young people through social media, I believe that I serve as a case study for its effectiveness in reaching target audiences. I am an undergraduate at Yale and a complete public health nerd. Although I mainly become involved in public health efforts by serving as a volunteer, I also use twitter and other social media as a way of connecting with public health professionals and catching up on new health programs and research. While participating on an online twitter chat about mental health awareness month I interacted with Dr. Payton and started to learn more about this project and its aims. As a young black women interested in health and more specifically women’s health, My Health Impact Network’s mission and goals really resonate with me.
Although young adults are very aware of HIV and other STD/STIs, it still is a very taboo topic in student communities. In my university of around 5000+ people, I do not know a single student living with HIV. This is not because there are not students living with the illness, but because it is still something that cannot be talked about in social circles. Many students received their main knowledge of STD/STIs through high school classes. Abstinence only focused or not, sexual education programs often use gruesome images and dire statistics of STD/STI cases which manifests in fear and stigma. Although the intention through these strategies is to encourage young adults to use condoms as protection, it instead creates silence and denial of STD/STIs. This stigma prevents young adults from talking about their diseases and the fear prevents people from regularly getting tested or having discussions with sexual partners.
Unfortunately, the stigma and fear are often carried to college and is not readdressed by university health programs. My freshman orientation focused mainly on acclimating to a new environment with alcohol and parties, which was entirely necessary and helpful, and a large emphasis on access to condoms. I am fortunate that my school has made access to condoms very easy by handing them out freely and putting them in the entryways of our dorms. It is important to recognize that not all schools provide these measures as demonstrated by the ban on free condoms at Boston College.
However, emphasis on condom use alone is not sufficient. Condoms are indeed the only way to minimize STD/STI contraction from a partner with unknown health status but condoms are sometimes not used or break. In these cases, sexual education mainly discusses the risk of pregnancy, but colleges must begin to openly talk about STD/STIs without stigma or shame. There has been significant progress in making sexual education much more comprehensive such as Get Yourself Tested month in April (http://www.itsyoursexlife.com/), and an emphasis on consent in sexual interactions, but there must be further and more long-term dialogue on removing the stigma from STD/STI contraction. In this education, I imagine more discussion about the statistics of STD/STI contraction and recovery on campus and clear information on the protocol for testing and treatment. In addition, health centers must be more accessible for immediate testing at the need of the student. These efforts must not follow the scare tactics of gruesome images and numbers of STD/STI deaths but rather an emphasis on what the resources actually provide.
How can we continue to remove the stigma and fear from STD/STIs while still focusing on the importance of protection? How can we foster more discussion of STD/STIs and personal experiences in student circles? Please continue the discussion in the comments.
Follow @myhealthimpact on Twitter.
Seyi Adeyinka is a student at Yale University. Seyi is interested in the barriers to health care access and how they manifest themselves in family planning and reproductive health at the local and international level. She is a Global Youth Advocacy Fellow for Planned Parenthood Federation of America and a Campus Action intern at her regional Planned Parenthood of Southern New England. She has also served as a Health Disparities Research Fellow at the University of Connecticut Health Center. At Yale, Seyi is a member of the Student Global Health and AIDS Coalition, Yale African Students Association, the Black Student Alliance, and is a Consent and Communication Educator.
Follow us at tumblr.myhealthimpactnetwork.org (Tumblr)
Follow us on Twitter @myhealthimpact
Share
June 03, 2013
How are you supporting national efforts to prevent cancer?
Texas A&M University
Doctoral Candidate
In light of the recent presidential proclamation by Obama for April to be observed as National Cancer Control Month, how are you supporting national efforts to prevent cancer?
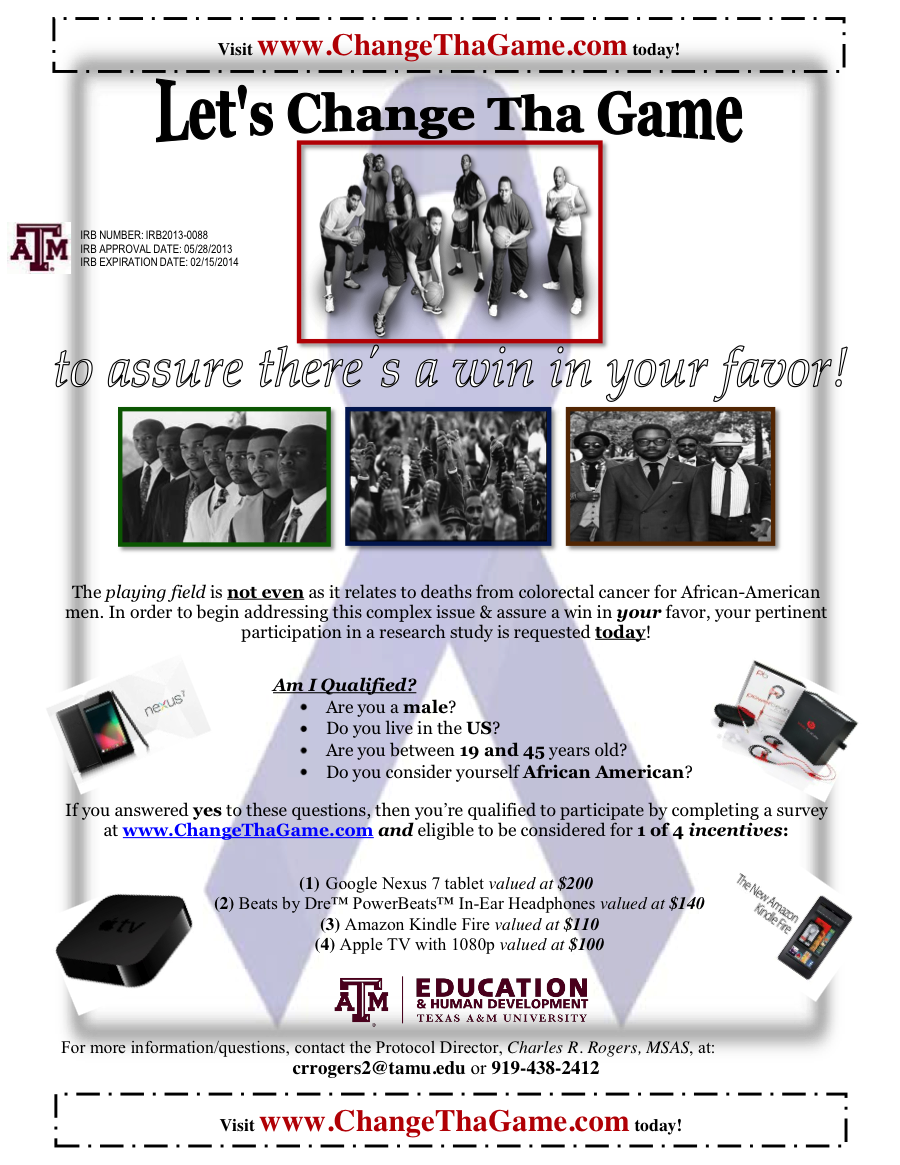
The playing field is not even as it relates to deaths from colorectal cancer (CRC) for African-American men. There is a critical need for exploring the poorly understood, complex factors that may shape intentions to screen for CRC among men who are younger than those traditionally assessed by health promotion researchers and clinicians (i.e., African-American men, ages 19-45). Ultimately, my proposed dissertation research will complement the mission of MyHealthImpactNetwork by contributing to solutions that eliminate disparities in health, cancer, and healthcare, moving closer to the long term goal of achieving health equity for all in the U.S.
If you are an African-American male between 19 and 45 years old living in the U.S., then you are qualified to participate by completing a brief survey at www.ChangeThaGame.com. If you are not qualified to participate, please spread the word via email, word of mouth, text message, Twitter, Facebook, LinkedIn, etc.! With your help, we can Change Tha CRC Game!
Follow us at tumblr.myhealthimpactnetwork.org (Tumblr)
Follow us on Twitter @myhealthimpact
Share
May 23, 2013
Performance and Images
Miami University
Doctoral Candidate
It is thought that the physical boundaries of white and black have long been broken down, for it has been well over fifty years since a little school girl named Linda Brown dreamt of walking to the all white school just a few blocks from her home. The color line has been crossed and blurred, leaving us all with a defocus aberration of race in America. The deracination is achieved through assimilation/integration, privileging whiteness and leaving the visages of your former self behind is compulsory.
Stripping away the identity of black other is a systematic process that functions in public spaces through hegemony, institutionally by the racialization of the legal system, and in private spaces due to the colonization of thoughts, which can be attributed to covert racist ideology and white supremacist schema (Fanon, 1963). While, being positioned in a post-civil rights space affords some safety and provides a path to American citizenship, no matter if the citizenship is temporary and is contingent on criteria that could and will change based on the whims of the oppressor, for the black other it is not without cost. Movement from explicit to implicit actions of racism has made racism almost unrecognizable, many whites and blacks alike would complicitly attend to their lives not contesting the structures of society that have informed their existence.
External forces such as schools, churches, organizations, community, and government act on the individual by plying pressure through hegemony molding the individual’s personhood (Cross, 1991). It is not to say that external forces are the sole determinant of self-concept, as if when born we begin as blank slates. Internal forces as well as external forces must be interrogated in a complex fashion to gain insight into black identity formation. Beginning with external forces, however leads to the internal in such that mental models are developed through environmental interaction. So, the child that is taught in school about the lack of black culture through the absences of black images and narratives infers the inferiority of blackness and develops self around this inference.
Likewise, the introduction of representations of blackness constructed through racist ontologies provides defined social and cultural position, clear roles for 'them and us'. Growing up black in white spaces supplies the black child with ready images to perform. The black boys and girls are cast in the roles early in school, defined by racist and classist ideology. Those blacks positioned in the middle class are given the role of black buddy and black lady or strong black woman, while, low-income blacks are pushed into the performativity of brut and jezebel.
The process of creating the other establishes the binary of us and them positioning each in opposition to the other. Tension arises from the polarity of us and them. The us strives to further distance themselves by mythologizing their history, telling stories of great odysseys, conquests, and inventions (Painter, 2010). In this new history the us begat the civilized world, founding rational thought, logic, and all that leads to a fully functional society. The them is constructed in juxtaposition to the us, being irrational, illogical, and destructive to society. It is within this context that African Americans operate, faced with daily marginalization.
In the eyes of the oppressor the other cannot aspire to great things, the history prorogated against them will not allow for greatness envisaged in the black body (Fanon, 1963). The struggle then becomes interpellation of white ideological beliefs and subjectification (Collins, 2001 & Butler, 1990). African Americans must cast off the remnants of the ‘authentic negro’ and engage in a performative act of self. The performance is castigated if the actors are not recognizable, their portrayal not believable or they choose to improvise. Living in a perpetuate world of performance due to the white gaze African Americans loss ‘self’ taking on the embodiment of the oppressor’s image of other. “In this American world, - a world which yields him no true self-consciousness, but only lets him see himself through the revelation of the other world (Du Bois, 1997).
References
Butler, J. (2006). Gender trouble: Feminism and the subversion of identity. Routledge classics. New York: Routledge.
Collins, P. (2004). Black sexual politics: African Americans, gender, and the new racism. New York: Routledge.
Cross, W. E. (1991). Shades of black: Diversity in African-American identity. Philadelphia: Temple University Press.
Du, B. W. E. B., Blight, D. W., & Gooding-Williams, R. (1997). The souls of Black folk. Boston: Bedford Books.
Fanon, F. (1991). The wretched of the earth. New York: Grove Weidenfeld.
Painter, N. I. (2010). The history of White people. New York: W.W. Norton.
Follow us at tumblr.myhealthimpactnetwork.org (Tumblr)
Follow us on Twitter @myhealthimpact
Share

May 06, 2013
The Evolution of a Sneakerhead
As the days dwindle away and graduation finds its way closer, a lot of thoughts have been running through my head. Thoughts primarily centered on my college experiences and how those moments have shaped me into the person I am today. Being a part of the myHealthImpact project has meant a lot to me, from gaining tangible skillsets to traveling across the country to promote our efforts. Although my obsession for simplicity and design drove my involvement with myHealthImpact, it was this representation of realizing a problem and attacking it head on with a unique solution that initiated my thoughts with respect to footwear.
As a child I was always fascinated with various types of sneakers. I wasn’t interested in wearing ‘regular’ or ‘basic’ shoes. I was more content with the latest and greatest Nikes, Jordan’s, and yes even Fila’s! I would beg my mom until she gave in and purchased my favorite pair of sneaks; but for some reason I was never completely satisfied. As the most expensive shoes felt uncomfortable and irritated me when I walked. This was evident because I had already been diagnosed with femoral antersion, or walking pigeon-toed, a common childhood orthopedic condition.
For a short time, I also wore shoes with braces, which I despised. While in middle school, I faced additional foot problems that made it difficult for my feet to stay on the foot bed of most sneakers. As a freshman at NCSU the foot problems ensued and further measures were taken such as creating a mold that I would wear in my shoes to provide comfort as I walked around campus. Currently, I have to engage in daily rituals by performing various foot exercises to ease the pains I may encounter during the day. Needless to say I have endured enough.
Despite my constant foot problems, for those who know me, I have been a lover of sneakers from the beginning of time. My devout following to rocking the latest kicks really took off when I entered college and met a small group of individuals who also shared this same passion. After accumulating dozens of shoes and even hosting the first ever sneaker showcase titled "Sneaks and Beat's' back in 2010, I still felt the need to do more. Now that I have officially hanged up my sneaks and done a lot of reflection, I have been toying with the idea of ending my retirement and refocusing my career on designing athletic footwear in conjunction with the medical field for optimal foot health.
Post graduation, I hope to take my experiences and turn it into a career filled with passion while helping others along the way. Thus, my involvement as an Undergraduate Researcher for this project has tremendously influenced me to pursue @myHealthImpact.
Follow us at tumblr.myhealthimpactnetwork.org (Tumblr)
Follow us on Twitter @myhealthimpact
Share
April 29, 2013
Response to Dr. Payton’s Blog Entitled “Sound Your Voices”
Jackson State University
Advisor: Dr. Lawrence T. Potter, Jr., Dean of the College of Liberal Arts
Why is it important for young black women to discuss the issue of HIV?
HIV should be an issue discussed among black women and the entire black community. The stats among black women are increasing at alarming rates. According to the C.D.C., most of the new cases that arise come from black women involved in heterosexual relationships. In addition, black women are still showing rates that are higher than any other race. Black women should become more vocal about not engaging in unprotected sexual relationships.
Furthermore, black women need to become adult advocates to educate each other about HIV and to become aware of the increased risk associated with the virus. However, black women must educate themselves first. Black women have to stop playing the victim role and start rising above the stats. Black women must stand as a united defense about the spread of HIV. Some ways that can help black women to become more vocal is increasing their knowledge about the virus, taking an initiative to protect yourself and others through getting tested, and sharing the information about HIV with friends and partners.
See myhealthimpactnetwork.org on the Web for other blogs, videos, newsletter signup and the newly released Android mobile app. Follow Dr. Payton and the research team @myhealthimpact on Twitter.
Follow us at tumblr.myhealthimpactnetwork.org (Tumblr)
Follow us on Twitter @myhealthimpact
Share
Page 14 of 18 pages ‹ First < 12 13 14 15 16 > Last ›
In Partnership with: National Science Foundation
Take Action, Get Tested: Find Your Local Testing Center Why Get Tested?